
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Fascia of neck
Semelhante a Fascia of neck (20)
Mais de mehermoinkhan
Mais de mehermoinkhan (20)
Último
Último (20)
Fascia of neck
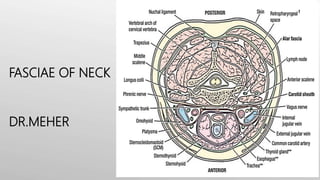
- 1. FASCIAE OF NECK DR.MEHER Fig 1.0 – Compartments of the neck
- 5. NECK • The neck is a tube providing continuity from the head to the trunk. It extends anteriorly from the lower border of the mandible to the upper surface of the manubrium of the sternum and posteriorly from the superior nuchal line on the occipital bone of the skull to the intervertebral disc between the CVII and TI vertebrae • four compartments provide longitudinal organization • The visceral compartment is anterior parts of the digestive and respiratory several endocrine glands. • The vertebral compartment is posterior and contains the cervical vertebrae, spinal cord, cervical nerves, and muscles associated with the vertebral column. • The two vascular compartments, one on each side, are lateral and contain the major blood vessels and the vagus nerve [X]. All these compartments are contained within unique layers of cervical fascia.
- 6. CUTANEOUS NERVES Skin over the Trapezius and back of the scalp supplied by posterior rami of cervical nerves 2-5.
- 7. Superficial fascia • Lies immediately next to the skin. • Consists of fats and connective tissue. • Contains cutaneous nerves, superficial veins, superficial lymph nodes and platysma. Fig 2.0 – The platysma muscle, located within thesuperficial cervical fascia.
- 8. Superficial Cervical Fascia The superficial cervical fascia lies between the dermis and the deep cervical fascia. It contains various structures: • Neurovascular supply to the skin • Superficial veins the external jugular vein • Superficial lymph nodes • Fat • Platysma muscle : thin but clinically imp, embebded in superficial fasica In obese individuals, extra fat is deposited in the superficial fascia, creating the ‘double chin’. The platysma muscle is situated on the anterior aspect of the neck. It has two heads, which originate from the fascia of the pectoralis major and deltoid. Fibers from the two heads cross the clavicle, and meet in the midline, fusing with the muscles of the face. • Develops from the 2nd pharyngeal arch and is supplied by branches of the facial nerve (CN VII). • Function: depresses the mandible Superficial fascia (details)
- 10. TRIBUTARIES OF EXTERNAL JUGULAR VEIN • Post. Auricular vein • Post. Division of RMV • Post. External Jugular vein • Transverse Cervical Vein • Supraclavicular Vein • Anterior Jugular Vein
- 13. Deep Cervical Fascia • Pretracheal layer : thin layer that is attached to the laryngeal cartilages. Surrounding the thyroid and parathyroid glands , forming a sheath , enclosing infrahyoid muscles Deep to the superficial fascia. the deep cervical fascia is organized into several distinct layers. These include: • an investing layer, Thick layer encircling the neck and enclosing trapezius and SCM • the prevertebral layer, thick layer passing like a septum across the neck behind the Pharynx and Esophagus , in front of the prevertebral muscles and vertebral column Fig 3.0 – Deep cervicalfascia.
- 14. • Deep cervical fascia also condenses around the common carotid and internal carotid arteries, internal jugular veins and vagus nerves to form the carotid sheath. The deep cervical fascia has several functions, including: • Support • Viscera (e.g. thyroid gland) • Muscles, Vessels and deep Lymph Nodes • Limit the spread of abscesses that result from infections • Slipperiness that allows structures in the neck to move and pass over one another without difficulty • Swallowing • Turning the head and neck Deep Cervical Fascia
- 16. Investing Layer The investing layer completely surrounds the neck. Attachments: Superior: attaches to the external occipital protuberance and the superior nuchal line. Anterior: attaches to the hyoid bone. Inferior: attaches to the spine and acromion of the scapula, the clavicle, and the manubrium of the sternum. Posterior: attaches along the ligamentum nuchae. Fig 3.0 – Investing layer.
- 17. • Where it meets the trapezius and sternocleidomastoid muscles, it splits into two, completely surrounding them. • The investing fascia can be thought of as a tube; with superior, inferior, anterior and posterior attachments • Component of the investing layer: • 2 muscles: SCM and trapezius • 2 salivary glands: Parotid and submandibular glands • 2 spaces: suprasternal and supraclavicular spaces Investing Layer
- 18. Clinical Relevance Because of the presence of thick tough parotid-masseteric fascia which covers the parotid gland swellings of the parotid gland (mumps, parotitis) are very painful. Picture 1.0 – Parotitis.
- 19. Pretracheal layer The pretracheal layer of fascia is situated anteriorly in the neck. It spans between the hyoid bone and the thorax, where it fuses with the pericardium. It can be anatomically divided into two parts: • Visceral – encloses the thyroid gland, trachea and esophagus. • Muscular – encloses the infrahyoid muscles. Fig 4.0 – Pretracheallayer.
- 20. Pretracheal layer • Posterior to the pharynx. the pretracheal layer is referred to as the buccopharyngeal fascia and separates the pharynx from the prevertebral layer. •The retropharyngeal space it is a potential space between the visceral part of the pretracheal layer anteriorly and the prevertebral layer posteriorly. • it is the largest, most important interfascial space in the neck - because it is the major route for spread of infection from the neck to the thorax.
- 21. Fig 4.1 – Buccopharyngealfascia. Pretracheal layer
- 22. Prevertebral fascia The prevertebral layer is a cylindrical layer of fascia that surrounds the vertebral column and the muscles associated with it. The prevertebral fascia is attached posteriorly along the length of the ligamentum nuchae, superiorly to the base of the skull and inferiorly to anterior longitudinal ligament of the vertebral column Fig 5.0 – Prevertebral layer.
- 23. Prevertebral fascia • The anterolateral portion of prevertebral fascia surrounds the brachial plexus and subclavian artery as they leave the neck, forming the axillary sheath.
- 24. Other component of the deep cervical fascia: • Carotid sheath: a condensation of the deep cervical fascia. Carotid sheath makes a free communication with the mediastinum of the thorax making a potential pathway for spread of infection and blood to the mediastinum. Contains: The common carotid artery and internal carotid artery Internal jugular vein The vagus nerve (CN X) • Visceral Fascia: encloses the pharynx and esophagus, larynx and trachea. • Potential Fascial Spaces: Alar and retropharyngeal spaces.
- 25. Clinical Relevance: Spread of infection! The deep fascial layers determine the direction in which abscesses in the neck may spread. If an infection occurs: • Between the Investing layer and the muscular part of the pretracheal surrounding the infrahyoid muscles, it will not spread beyond the manubrium. • Between the Investing and visceral Pretracheal layers, it can spread into the thoracic cavity anterior to the pericardium.
- 26. Clinical Relevance: Spread of infection! Fig 6.0 – Spread of infection.
- 27. • Pus from an abscess lying behind the Prevertebral layer of deep cervical fascia may extend laterally in the neck. May perforate the fascial layer and enter the retropharyngeal space. This will produce a bulge (retropharyngeal abscess) in the pharynx, resulting in dysphasia (difficulty swallowing) and dysphonia (difficulty speaking) Clinical Relevance: Spread of infection! Fig 6.0 – retropharyngealabscess.