Classification and Treatment of Periodontal Pockets
•Transferir como DOCX, PDF•
42 gostaram•9,804 visualizações

Lecture about Periodontal pocket, Kohat, Pakistan

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Classification and Treatment of Periodontal Pockets
Semelhante a Classification and Treatment of Periodontal Pockets (20)
Mais de Dr.Jaffar Raza BDS
Mais de Dr.Jaffar Raza BDS (20)
Último
Último (20)
Classification and Treatment of Periodontal Pockets
- 1. Dr Jaffar Raza Syed Page 1 Periodontal Pocket
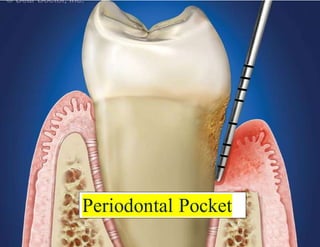
- 2. Dr Jaffar Raza Syed Page 2 Periodontal Pockets “Pocket can be defined as deepening of the gingival sulcus.” Pseudo-pocket Coronal migration of the marginal gingiva True pocket Deepening due to apical migration of the junctional epithelium
- 3. Dr Jaffar Raza Syed Page 3
- 4. Dr Jaffar Raza Syed Page 4 ClassificationOf Pockets 1. Depending upon its morphology a. Gingival/false/relative pocket. b. Periodontal/absolute/true pocket. c. Combined pocket.
- 5. Dr Jaffar Raza Syed Page 5 2. Depending upon its relationship to crestal bone a. Suprabony/supracrestal/supra-alveolar pocket. b. Infrabony/intrabony/subcrestal/intra-alveolar pocket.
- 6. Dr Jaffar Raza Syed Page 6 3. Depending upon the number of surfaces involved: a. Simple pocket—involving one tooth surface. b. Compound pocket—involving two or more tooth surfaces. c. Complex pocket—where the base of the pocket is not in direct communication with the gingival margin. It is also known as spiral pocket.
- 7. Dr Jaffar Raza Syed Page 7 4. Depending upon the nature of the soft tissue wall of the pocket a. Edematous pocket. b. Fibrotic pocket. 5. Depending upon the disease activity a. Active pocket. b. Inactive pocket.
- 8. Dr Jaffar Raza Syed Page 8 CLINICAL FEATURES Enlarged, bluish-red marginal gingiva with a ‘rolled’ edge A break in the faciolingual continuity of the interdental gingiva. Shiny, discolored and puffy gingiva associated with exposed root surfaces. Gingival bleeding, purulent exudate from the gingival margin. Mobility,extrusionand migrationof teeth. The development of diastema where none had existed previously.
- 9. Dr Jaffar Raza Syed Page 9 Symptoms Localized pain or a sensationof pressure in the gingival after eating, which gradually diminishes. A foul taste in localized areas. A tendency to suck material from the interproximal spaces. Radiating pain “deep in the bone”. A “gnawing’ feeling or feeling of itching in the gums. The urge to dig a pointed instrument into the gums and relief is obtained from the resultant bleeding. Patient complains that food “sticks between the teeth” or that the teeth “feel loose”or a preference to “eat on the other side.” Sensitivity to heat and cold; toothache in the absence of caries.
- 10. Dr Jaffar Raza Syed Page 10
- 11. Dr Jaffar Raza Syed Page 11 PATHOGENESIS
- 12. Dr Jaffar Raza Syed Page 12
- 13. Dr Jaffar Raza Syed Page 13
- 14. Dr Jaffar Raza Syed Page 14
- 15. Dr Jaffar Raza Syed Page 15 Changes in the SoftTissue Wall blood vessels are engorged and dilated connective tissue is edematous and densely infiltrated with plasma cells (80%), lymphocytes and PMNL epithelium along the lateral wall of the pocket presents striking proliferative and degenerative changes epithelial projection extends deep into the connective tissue and also extends further apically than the junctional epithelium.
- 16. Dr Jaffar Raza Syed Page 16 The epithelium is infiltrated with leukocytes and other inflammatory cells. Degeneration and necrosis of the epithelium leading to ulceration of the epithelium and exposure of the underlying connective tissue. Bacterial invasion along the lateral and apical areas of the pocket. Some bacteria traverse the basement lamina and invade the subepithelial connective tissue
- 17. Dr Jaffar Raza Syed Page 17 Pocket contents Mainly debris consisting of microorganisms and their products (enzymes, endotoxins, and other metabolic products), gingivalfluid, food remnants, salivary mucin, desquamatedepithelial cells, leukocytes. Plaque-covered calculus projecting from tooth surface. Purulent exudate consists of living, degenerated, and necrotic leukocytes; living and dead bacteria; serum
- 18. Dr Jaffar Raza Syed Page 18 Zones In The Base Of A Periodontal Pocket
- 19. Dr Jaffar Raza Syed Page 19 Relation of Loss of Attachment and Bone Loss to Pocket Depth Pocket of same depth may be associated with different degree of attachment loss. Pocket of different depth may be associated with same amount of attachment loss. Area between the base of the pocket and the alveolar bone is always constant. The radius of action of the plaque bacteria is 0.5 to 2.7 mm
- 20. Dr Jaffar Raza Syed Page 20
- 21. Dr Jaffar Raza Syed Page 21 TREATMENT OF PERIODONTAL POCKET I. Treatment of pocket depends on the type of pocket
- 22. Dr Jaffar Raza Syed Page 22 II. Treatment of suprabony and infrabony pockets
- 23. Dr Jaffar Raza Syed Page 23 New attachment techniques: It offers ideal result by reuniting the gingiva to the tooth at a position Coronal to the base of pre-existing pocket. Here all the structures of lost periodontium are restored. Following are the techniques for new attachment: Non-graft associated new attachment procedures. Graft associated new attachment procedures. Combined techniques.
- 24. Dr Jaffar Raza Syed Page 24 Removal of pocket wall by, 1. Retraction or shrinkage, e.g. scaling and root planing. 2. Surgical removal by gingivectomy or by means of an undisplaced flap. 3. Apical displacement of pocket wall by apically displaced flap. Removal of the tooth side of the pocket, by tooth extraction or partial tooth extraction such as hemisection or root resection. Bicuspidization